
Compare mupirocin and fusidic acid — evidence, safety, and barrier-conscious use to manage bacterial skin conditions effectively.
Two Trusted Topicals, One Critical Choice
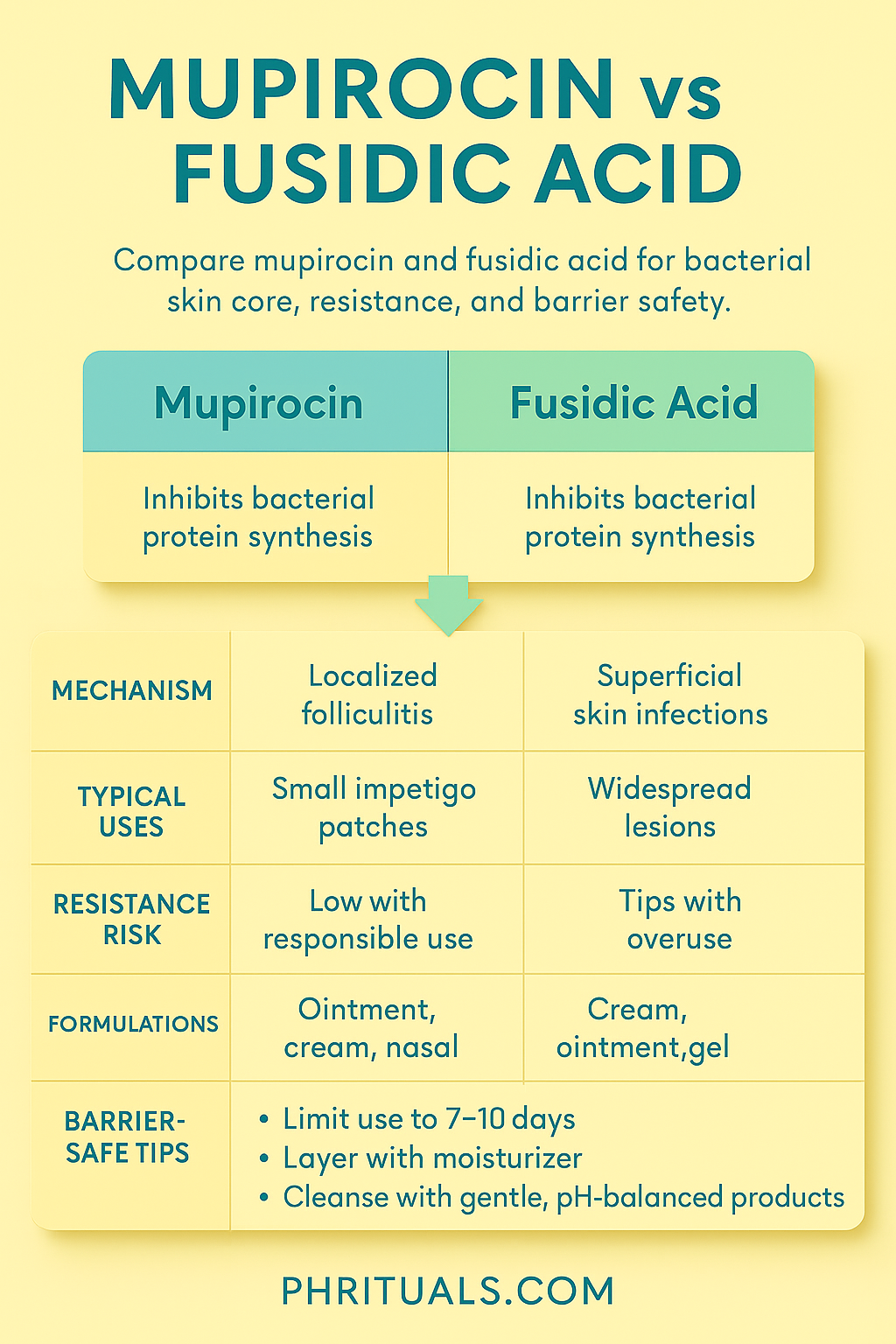
When bacterial skin infections like folliculitis, mild impetigo, or infected acne lesions appear, two topical antibiotics often come up: mupirocin and fusidic acid. Both are clinically effective, but they work differently, have unique resistance risks, and require careful integration into barrier-safe routines.
This article examines what the evidence says about each, so you can make informed, dermatologist-aligned choices.
Direct Answer
Mupirocin and fusidic acid are both effective topical antibiotics for bacterial skin conditions, but they serve different purposes:
- Mupirocin is typically first-line for localized infections, especially when Staphylococcus aureus is involved.
- Fusidic acid is equally effective but often reserved where resistance patterns or specific bacterial strains warrant its use.
Mechanisms of Action
Mupirocin
- Target: Inhibits bacterial protein synthesis by binding to isoleucyl-tRNA synthetase.
- Spectrum: Primarily Staphylococcus aureus and Streptococcus pyogenes.
- Use Cases: Infected eczema patches, localized folliculitis, mild impetigo, and sometimes acne lesions complicated by bacterial overgrowth.
Fusidic Acid
- Target: Inhibits bacterial protein synthesis by binding elongation factor G.
- Spectrum: Broad Staphylococcus coverage and some gram-positive bacteria.
- Use Cases: Surface infections, particularly in settings where mupirocin resistance is rising.
Evidence-Based Efficacy
| Attribute | Mupirocin | Fusidic Acid |
|---|---|---|
| Antibacterial Strength | High against S. aureus and S. pyogenes | High against S. aureus; moderate for other gram-positive bacteria |
| Time to Results | Rapid improvement within 3–5 days | Similar 3–5 day improvement window |
| Resistance Risk | Lower but rising with misuse | Moderate, particularly with prolonged unsupervised use |
| Formulations | Ointment, cream, nasal forms | Cream, ointment, gel |
Barrier & PIH Considerations
- Both antibiotics are well-tolerated, but:
- Overuse may disrupt the microbiome and weaken barrier resilience.
- Irritation can lead to post-inflammatory hyperpigmentation (PIH) in melanin-rich skin if not supported with barrier repair products.
- Always pair topical antibiotics with a gentle cleanser and ceramide-rich moisturizer to minimize disruption.
When to Use Each
| Scenario | Recommended Active | Why |
|---|---|---|
| Localized folliculitis or small impetigo patches | Mupirocin | Fast action, low irritation |
| Widespread superficial infection | Fusidic Acid | Broader coverage, better spreadability |
| Known mupirocin resistance | Fusidic Acid | Maintains efficacy where mupirocin fails |
| Nasal carriage of S. aureus (per derm advice) | Mupirocin (nasal formulation) | Targeted eradication |
Safe Integration into Skincare
- Cleanse gently: Use pH-balanced syndet cleansers to prep the skin without stripping.
- Apply sparingly: A thin layer to the affected area 2–3 times daily, unless otherwise advised by a dermatologist.
- Protect barrier: Layer ceramide-rich moisturizers to prevent dryness and irritation.
- Use only as prescribed: Limit use to 7–10 days to prevent resistance.
- Monitor for reactions: Redness, itching, or delayed healing should prompt a medical review.
Resistance Awareness
- Both mupirocin and fusidic acid are prone to resistance when overused.
- To reduce this risk:
- Use for short, targeted courses.
- Avoid applying to large, uninfected areas.
- Pair with proper hygiene and, where needed, oral antibiotics prescribed by a physician.
Key Takeaway
- Mupirocin is best for targeted, localized infections with low resistance risk.
- Fusidic acid is valuable for broader coverage but should be used cautiously to avoid resistance.
- Both can be safely integrated into barrier-focused routines when used responsibly and paired with gentle, supportive skincare.
References
- Koning, S., et al. (2014). Mupirocin for bacterial skin infections. Cochrane Database of Systematic Reviews, 2014(11), CD002749.
- Røttingen, J. A., et al. (2017). Resistance trends in topical antibiotics. Journal of Antimicrobial Chemotherapy, 72(4), 984–991.
- Verhoeven, P. O., et al. (2016). Topical fusidic acid: Clinical applications and resistance patterns. Clinical Microbiology and Infection, 22(5), 356–362.
- NICE. (2023). Impetigo: Antimicrobial prescribing. Retrieved from https://www.nice.org.uk
- American Academy of Dermatology. (2024). Guidelines for management of superficial skin infections.